
Written and medically reviewed by Chris Woods, MSN, APRN, FNP-C
This article reflects Chris’s real clinical experience treating common urgent-care conditions through NPCWoods Telemedicine. Content is reviewed for accuracy, updated over time, and paired with clear guidance on when text-based care is appropriate and when in-person care matters more.
Licensed Nurse Practitioner. Licensed in AZ, CO, GA, ID, IA, MT, NV, NM, NC, OR, UT. NPI 1285125468.
Published April 10, 2026. Last reviewed and updated April 24, 2026.
You text Chris directly. No AI triage, no call center, and no copy-paste handoff between strangers.
This article is educational only. For chest pain, trouble breathing, severe dehydration, confusion, or other emergencies, call 911 or seek urgent in-person care.

What Is Async Telemedicine and How Does It Work?
Async telemedicine is healthcare by text message — you send your symptoms, a licensed provider reviews them, and prescriptions go to your pharmacy. No video call. No appointment. No waiting room. The clinical term is “asynchronous telehealth,” and it is the fastest-growing model in outpatient medicine for one simple reason: many common conditions do not require a face-to-face exam to diagnose and treat safely.
I’m Chris Woods, a double board-certified Nurse Practitioner, and I run NPCWoods — an async telemedicine practice that treats patients across multiple states entirely by text. I built this practice because I watched too many people sit in urgent care for two hours with a UTI that could have been handled in ten minutes. Let me walk you through exactly how async telemedicine works, what the clinical evidence says, and when it makes sense for you.
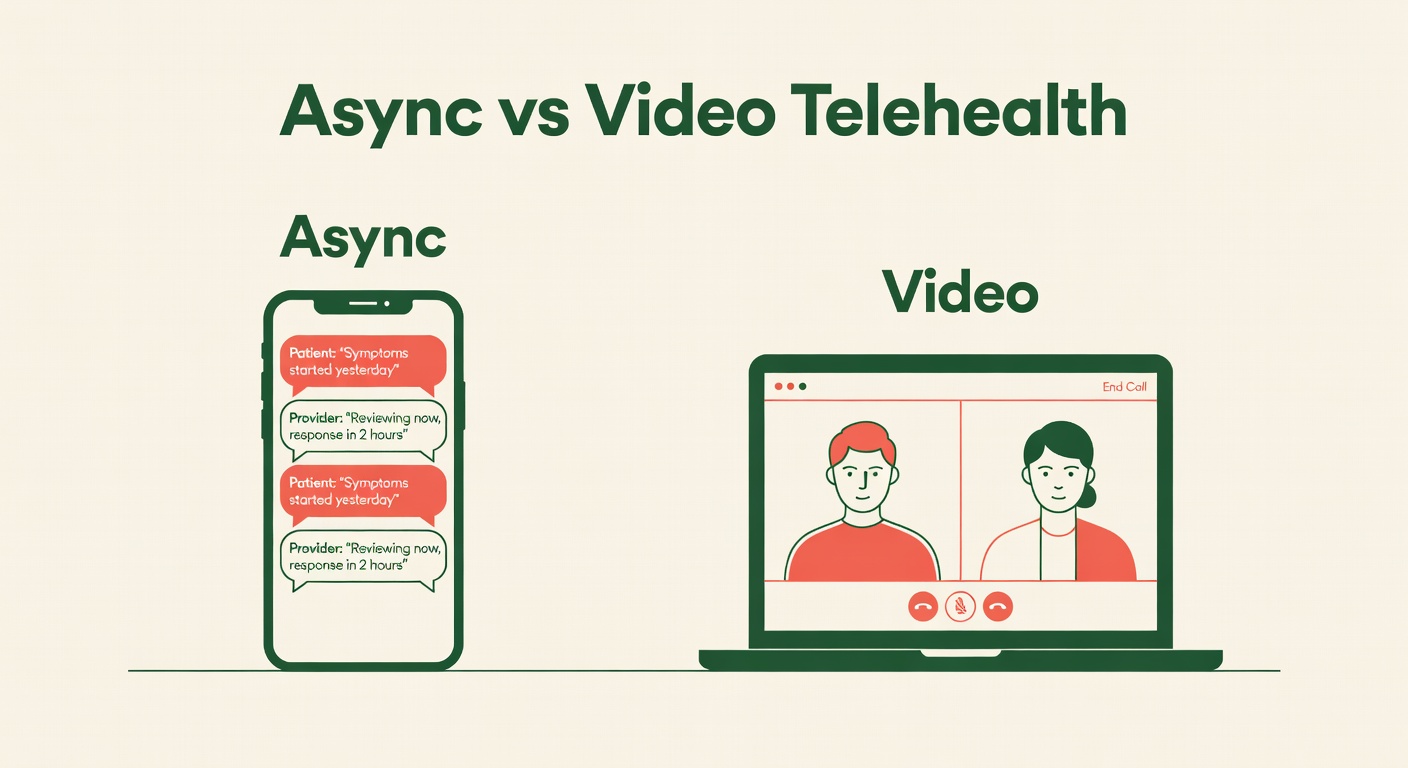
How Async Telemedicine Differs from Video Telehealth
Most people hear “telehealth” and picture a video call with a provider. That is synchronous telehealth — both parties have to be online at the same time. Async telemedicine removes that constraint entirely.
| Async (Text-Based) | Synchronous (Video Call) | |
|---|---|---|
| Scheduling | None — text anytime, 24/7 | Book a time slot |
| Wait time | Typically under 2 hours | 15–45 min in virtual waiting room |
| Privacy | Text from anywhere — no one overhears | Need a quiet, private room |
| Documentation | Full written record by default | Provider writes notes after |
| Best for | Straightforward conditions with clear symptoms | Complex or visual assessments |
The key difference is efficiency. Async telemedicine works on your schedule, not the clinic’s. You describe your symptoms when it is convenient for you — during your lunch break, after the kids are in bed, at 2 a.m. when that UTI wakes you up. A licensed provider reviews everything and responds with a treatment plan or follow-up questions.
What Conditions Can Async Telemedicine Treat?
Async telemedicine is designed for common, symptom-driven conditions where the diagnosis can be made from a detailed history. These are conditions that clinicians diagnose every day based primarily on what the patient tells them — not on what they see through a stethoscope. Here is what NPCWoods treats via async:
- Urinary tract infections (UTIs) — burning, frequency, urgency
- Sinus infections — facial pressure, discolored drainage, 10+ days of congestion
- Strep throat — sore throat, fever, no cough (Centor criteria)
- Ear infections — ear pain, pressure, recent upper respiratory symptoms (when history strongly suggests diagnosis; some cases may require in-person evaluation)
- Pink eye (conjunctivitis) — redness, discharge, crusting
- Cold sores — tingling, blistering on lips
- Flu — rapid onset fever, body aches, fatigue (within 48 hours for antivirals)
- Yeast infections — itching, discharge, prior history
When Async Is Not the Right Choice
Async telemedicine is not appropriate for emergencies, chest pain, difficulty breathing, sudden severe headaches, or any condition that requires a physical examination. If a provider determines during an async visit that you need in-person care, they will tell you — and you will not be charged. Responsible async practices build that safety net into the model.
The Clinical Evidence Behind Async Diagnosis
This is not a shortcut — it is evidence-based medicine. Major clinical guidelines already support symptom-based diagnosis for these conditions:
- UTIs: The Infectious Diseases Society of America (IDSA) guidelines support empiric treatment of uncomplicated UTIs in women based on symptom history alone — no lab required for classic presentations.
- Sinus infections: CDC and IDSA guidelines recommend clinical diagnosis of acute bacterial sinusitis based on symptom duration and pattern. Imaging is not recommended for routine cases.
- Strep throat: The Centor/McIsaac scoring criteria use symptom history (fever, tonsillar exudates, no cough, tender anterior cervical nodes) to stratify strep risk and guide treatment decisions.
- Flu: CDC guidelines support empiric antiviral treatment based on clinical presentation during flu season, particularly within the first 48 hours of symptom onset.
In other words, for these specific conditions, the clinical standard of care already relies heavily on what the patient reports. Async telemedicine simply moves that conversation from a physical exam room to a secure text thread. The clinical reasoning is the same. Learn more about our clinical experience and credentials.
How NPCWoods Async Telemedicine Works: 5 Steps
Here is exactly how it works at NPCWoods:
- Text us at (480) 639-4722. Tell us what is going on — your symptoms, how long they have lasted, any medications you are taking, and any relevant history.
- A licensed NP reviews your message. I personally read every intake. If I need more detail, I will ask targeted follow-up questions via text.
- You get a clinical assessment. I explain what I believe is going on, why I believe it, and what the treatment plan is — all in plain language you can read back anytime.
- Prescriptions are sent to your pharmacy. You pick a pharmacy, I send the prescription electronically. Most patients have medication in hand within hours.
- Follow-up is included. If symptoms do not improve, you text back. No additional charge for follow-up on the same visit.
The entire visit is $59. That is it. No hidden fees, no membership, no subscription. One flat rate per visit. Check our FAQ for the most common questions.
Async Telemedicine vs. Urgent Care vs. Emergency Room
Knowing where to go matters. Here is a straightforward guide, and we break this down further on our telehealth vs. urgent care page:
| Setting | Best For | Typical Cost | Wait Time |
|---|---|---|---|
| Async Telemedicine | UTIs, sinus infections, strep, ear infections, pink eye, cold sores, flu, yeast infections | $59 | Minutes to 2 hours |
| Urgent Care | Sprains, minor lacerations, conditions needing physical exam or labs | $150–$300+ | 45 min – 3 hours |
| Emergency Room | Chest pain, difficulty breathing, severe injury, stroke symptoms | $500–$3,000+ | 1–6+ hours |
Async telemedicine is not trying to replace urgent care or the ER. It is designed to handle the conditions that never needed a waiting room in the first place. If you have a straightforward UTI, you do not need to sit under fluorescent lights next to someone with a broken wrist. You need antibiotics — and you can get them from your couch.
Why Async Telemedicine Is the Future of Common-Condition Healthcare
Healthcare is moving toward meeting patients where they are, and most patients are on their phones. Async telemedicine represents a fundamental shift in how routine care is delivered:
- Access: Patients in rural areas, working parents, night-shift workers, and anyone without flexible scheduling can get care without taking time off work.
- Speed: Most async visits at NPCWoods are completed in under two hours from first text to prescription sent.
- Transparency: Flat-rate pricing means you know the cost before you start. No surprise bills, no copay confusion.
- Quality: A written text thread creates a complete medical record of every question asked and every answer given. Nothing gets lost in translation.
- Patient comfort: Some people find it easier to describe sensitive symptoms — like UTI or yeast infection details — over text than face-to-face. That honesty leads to better care.
The pandemic proved that telehealth works. Async telemedicine is the next step — stripping away the parts that still feel like a clinic visit (scheduling, waiting, video setup) and keeping only what actually matters: a licensed provider making a clinical decision based on your symptoms.
Ready to Try Async Telemedicine?

If you are dealing with a UTI, sinus infection, strep throat, or any of the conditions listed above, you do not need to wait for an appointment. You do not need to drive anywhere. You just need your phone.
Text us right now: (480) 639-4722
$59 per visit. No subscription. No appointment. Just tell us what is going on and we will take it from there.
Sources & Clinical References
This article is for educational purposes only and does not replace professional medical advice. Async telemedicine is appropriate for many common conditions but is not a substitute for emergency or in-person care when clinically indicated. If you are experiencing a medical emergency, call 911. For non-emergency symptoms, text (480) 639-4722 to speak with a licensed nurse practitioner.
- Gupta K, Hooton TM, Naber KG, et al. “International Clinical Practice Guidelines for the Treatment of Acute Uncomplicated Cystitis and Pyelonephritis in Women: A 2010 Update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases.” Clinical Infectious Diseases. 2011;52(5):e103-e120. doi:10.1093/cid/ciq257
- Chow AW, Benninger MS, Brook I, et al. “IDSA Clinical Practice Guideline for Acute Bacterial Rhinosinusitis in Children and Adults.” Clinical Infectious Diseases. 2012;54(8):e72-e112. doi:10.1093/cid/cir1043
- McIsaac WJ, White D, Tannenbaum D, Low DE. “A Clinical Score (Modified Centor) to Reduce Unnecessary Antibiotic Use in Patients Presenting with Sore Throat in Primary Care.” Canadian Medical Association Journal. 1998;158(1):75-83.
- Grigoryan L, Trautner BW, Gupta K. “Diagnosis and Management of Urinary Tract Infections in the Outpatient Setting: A Review.” JAMA. 2014;312(16):1677-1684. doi:10.1001/jama.2014.12842
- Centers for Disease Control and Prevention. “Antibiotic Prescribing and Use: Sinus Infection (Sinusitis).” Updated 2024. cdc.gov
- Centers for Disease Control and Prevention. “Influenza Antiviral Medications: Summary for Clinicians.” Updated 2024. cdc.gov
